Article
Addressing patellofemoral pathology: Biomechanics and classification
There is no clear consensus about which therapiesshould be used for the various underlying pathologies that lead topatellofemoral problems. The major distinction in classification isbetween patellofemoral compression syndrome and patellofemoralinstability. Patients with the former are concerned primarily withpain; those with the latter have instability or pain or both. Patellarpain may manifest in the parapatellar area or radiate to the back ofthe knee. Persons' differing activity and conditioning levels maylead to patellofemoral pain variability. Patients with patellar instabilityinclude those with recurring frank patellar dislocations andthose with symptoms of subluxation. Patients who have patellar instabilitypresent with tears of the medial patellofemoral ligament;this is the "essential lesion" for patellar dislocation. (J MusculoskelMed. 2008;25:297-300)
ABSTRACT: There is no clear consensus about which therapies should be used for the various underlying pathologies that lead to patellofemoral problems. The major distinction in classification is between patellofemoral compression syndrome and patellofemoral instability. Patients with the former are concerned primarily with pain; those with the latter have instability or pain or both. Patellar pain may manifest in the parapatellar area or radiate to the back of the knee. Persons' differing activity and conditioning levels may lead to patellofemoral pain variability. Patients with patellar instability include those with recurring frank patellar dislocations and those with symptoms of subluxation. Patients who have patellar instability present with tears of the medial patellofemoral ligament; this is the "essential lesion" for patellar dislocation. (J Musculoskel Med. 2008;25:297-300)
Many classification systems have been devised to help clinicians, both surgeons and nonsurgeons, understand and properly address patellofemoral dysfunction. However, no system has become uniformly accepted. As a result, there is no clear consensus about which therapeutic measures should be used for the various underlying pathologies that lead to patellofemoral problems.
In our opinion, grouping patients with patellofemoral dysfunction according to treatment strategy produces the most practical classification system. The major distinction to be made is between patellofemoral compression syndrome and patellofemoral instability.
Patients with patellofemoral compression syndrome present primarily with pain. They tend to have tight tissue that leads to excessive pressure between the patella and trochlea. Patients usually are treated with nonoperative measures, although operative procedures may be indicated.
Patients with patellofemoral instability complain of instability or pain or both. Instability concerns may manifest as frank patellar dislocation or may be more subtle (eg, a patient with subluxation may feel the knee cap "slip and slide"during activities).Pain complaints are similar to those made by patients who have patellofemoral compression syndrome. First-time dislocation typically is managed nonoperatively if there is no loose body or osteochondral lesion; recurring instability is more likely managed with surgery.
This 3-part article discusses the diagnosis and management of patellofemoral pathology. In this first part, we describe the biomechanics of patellofemoral dysfunction and classification of problems for determining proper treatment. The second part, to appear in a later issue of this journal, will focus on the physical examination. In the third part, we will review various approaches to treatment.
BIOMECHANICS
When the knee is in full extension, the patella sits on the supratrochlear fat pad lateral to the trochlea. As the knee moves from an extended to a flexed position, the contact area of the patella onto the trochlea shifts from distal to proximal. For example, the trochlea articulates with the distal patellar and midpatellar articular surfaces at 10° to 20° and at 30° to 60° of knee flexion, respectively.1 This concept is important when a physical therapy prescription is written-the location of chondral damage affects the range of motion in which strengthening exercises are performed.
If the tibial tubercle is significantly lateralized compared with the trochlea, the patellar tendon may exert a laterally directed force on the patella. This force vector may be quantified with CT scanning or clinically with measurement of the Q angle (the angle formed between the tibial tubercle, center of the patella, and anterior superior iliac spine; a Q angle greater than 20° is considered abnormal) (Figure 1). Other force producing factors that result in a laterally directed vector include femoral rotation, excessive femoral anteversion, and tight lateral retinacular tissue.


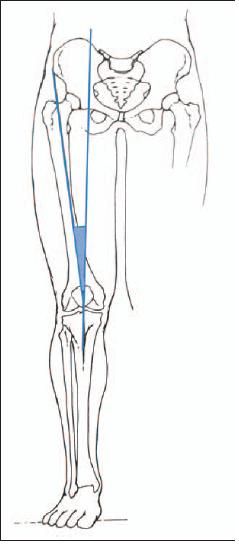
Figure 1 –
In patients with patellar instability, the patellar tendon may exert a laterally directed force on the patella. This force vector may be quantified with measurement of the Q angle, the angle formed between the tibial tubercle, center of the patella, and anterior superior iliac spine; a Q angle greater than 20° is abnormal.
SYMPTOMS
Pain
Patellar pain may manifest in the parapatellar area (just medial or lateral to the patella) or radiate to the back of the knee. Some authors have stated that they can distinguish between patellofemoral compression syndrome and patellofemoral instability based on the location of pain (personal communication, J. P. Fulkerson, 2006). They relate lateral parapatellar pain with compression and medial parapatellar pain with instability. We have not found this association to be uniformly true.
Patients may present with posterior knee pain. In some cases, they enter a clinic with MRI results demonstrating a Baker cyst. Discussing the diagnosis of patellofemoral disease with these patients becomes challenging because they are convinced that the pain is caused by the cyst.
Dye2 attributed day-to-day changes in a patient with patellofemoral pain to a loss of patellar and peripatellar tissue homeostasis. He coined the term "envelope of load acceptance," or "envelope of function," to account for why the same load may lead to patellofemoral pain in one person and not in another or even lead to pain in the same person at one time but not at another.3
The envelope of load acceptance is related to overuse or a discrete, single event that is excessive. The loads transmitted across the knee vary according to complex factors, such as the dynamic center of gravity, rate of load application, and angles of flexion and rotation.4 For example, a person who is out of shape tries to climb several flights of stairs for a workout. This level of activity may be beyond the range of acceptable physiological load across the joint, and patellofemoral pain may result. In this case, the pain is a result of overuse, although patellofemoral pain also may be caused by a discrete event (eg, twisting a knee).
Another person does the same workout by climbing several flights of stairs but is well conditioned. In this person, this level of activity may be within the range of acceptable physiological load across the joint and patellofemoral pain might not result.
Thus, persons' differing activity and conditioning levels may lead to patellofemoral pain variability. More important, the envelope of load acceptance or function narrows after an injury, such that a previously well-tolerated activity now causes pain. Because of the variances, rehabilitation with physical therapy should be tailored to individual patients.
Emphasizing this concept to patients is useful. A patient often is told that he or she has arthritis "under the kneecap" or that the kneecap has undergone wear and tear. The patient's immediate response may be, "But I didn't have pain before doing (a specific) activity." An explanation that is easier for patients to understand is that there is irritation between the kneecap and the thigh bone groove (trochlea) on which the kneecap travels and that the patellofemoral pain resolves when the irritation has resolved.
Instability
Patients with patellar instability include those with recurring frank patellar dislocations and those with symptoms of subluxation. With subluxation, complaints of the patella being "loose" or slipping and sliding usually are made when it is in a position in which the femur internally rotates on a fixed, externally rotated tibia. Because this position is similar to that in which anterior cruciate ligament (ACL) tears occur, a clinician may mistake a patellar dislocation for an ACL tear.
Patients who have patellar instability present with tears of the medial patellofemoral ligament (MPFL). There may be exacerbating bony malalignment or dysplasia; patella alta; Q angle greater than 20º; tibial tubercle to trochlear groove distance greater than 15 mm; or trochlear dysplasia. Longterm instability may lead to tissue contracture that may overlap with descriptions attributed to compression syndrome (tight lateral retinaculum), which is the result of a chronically displaced patella. Patients may describe symptoms of instability without complaints of pain.
Patients who have patellar instability may report episodes of pain with acute patellar subluxation or dislocations. The pain may result from an acute inflammatory process with soft tissue injury or bone injury (eg, edema/bruise) or from an osteochondral fracture. A bone bruise typically is seen in the medial facet of the patella or in the lateral femoral condyle.
Patellar subluxation is not synonymous with knee buckling, or "giving way," which occurs with patellofemoral pain-because of pain inhibition-as it does with meniscal pathology. In contrast, patellar subluxation or instability is a sense the patient has that the kneecap is slipping and sliding.
Nomura and associates5 reported that 95% of first-time patellofemoral dislocators sustained a cartilage injury; 72% demonstrated osteochondral patellar fragments, and 26% had articular damage of the lateral femoral condyle. Several authors stated that the diagnosis was made with preoperative x-ray films in only 32% to 80% of patients with osteochondral fractures.6,7
The MPFL is the "essential lesion" for patellar dislocation (Figure 2).8 The origin is in an area between the medial femoral epicondyle and the adductor tubercle. The insertion is at the proximal/ medial aspect of the patella. The MPFL is superficial to the joint synovium.


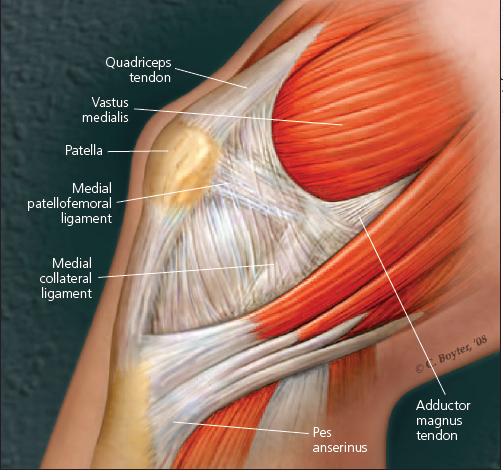
Figure 2 –
The medial patellofemoral ligament (MPFL) is the "essential lesion" for patellar dislocation. The origin is between the medial femoral epicondyle and the adductor tubercle.The insertion is at the proximal/medial aspect of the patella. The MPFL is superficial to the joint synovium.
Patellar dislocation risk factors
In a prospective study that evaluated a cohort of first-time patellofemoral dislocators and recurrent dislocators, Fithian and colleagues9 showed a 17% risk of a repeat dislocation after the first dislocation (similar to previously published results) and a 49% risk with a history of more than 1 previous dislocation. At 2- to 5-year follow-up, patients with a history of more than 1 dislocation had a 30% chance of contralateral patellofemoral dislocation, compared with 9% in patients with only 1 dislocation. Females aged 10 to 17 years were at highest risk for redislocation in both the first time and recurrent dislocator cohorts. MRI findings at the time of the first dislocation associated with future recurrences are lack of edema of the vastus medialis obliquus muscle, MPFL midsubstance injuries, and MPFL femoral attachment injuries.
The chances of sustaining a dislocation were 6 times higher with a history of patellofemoral dislocation and 4 times higher with a family history of this dislocation. They were 15 times higher with a history of developmental dysplasia of the hip.
Larsen and Lauridsen10 reported that patella alta and lateral patellar displacement are significantly more common in patients with patellar dislocations who deny a history of trauma than in those who attribute the dislocation to trauma. They also reported that patients who were younger than 20 years when they sustained their first patellofemoral dislocation tend to redislocate more than patients who were older than 20 years.
Generalized ligamentous laxity, initially described by Carter and Wilkinson,11 has been shown to be a predictor of poor clinical outcome after realignment surgeries, procedures that aim to reef or tighten tissue or alter the vector of force.12,13 The signs include doughlike skin consistency, elbow hyperextension, the ability to fold the thumb to reach the volar forearm surface, knee hyperextension, and the ability to touch the palms on the ground with the knees kept in extension.
Compression
Patellofemoral compression syndrome results from excessive tension or compression of soft tissue structures; there may be exacerbating bony malalignment. For example, a tight lateral retinaculum places the patella at risk for facing excessive compressive forces against the trochlea as the knee is flexed; if a shortened iliotibial band pulls posteriorly on the shortened lateral retinaculum, the patella faces even more profound compressive forces.14 These tightened structures lead to lateral tracking of the patella. In addition, a tight hamstring and tight gastrocnemius accentuate lateral patella tracking by increasing the dynamic Q angle.
References:
References
1.
Goodfellow J, Hungerford DS, Zindel M. Patello-femoral joint mechanics and pathology. Functional anatomy of the patello-femoral joint.
J Bone Joint Surg.
1976;58B:287-290.
2.
Dye SF. The pathophiology of patellofemoral pain: a tissue homeostasis perspective.
Clin Orthop Relat Res.
2005;436:100-110.
3.
Dye SF. The knee as a biologic transmission with an envelope of function: a theory.
Clin Orthop Relat Res.
1996;325:10-18.
4.
Dye SF. The pathophysiology of patellofemoral pain: a tissue homeostasis perspective.
Clin Orthop Relat Res.
2005;436:100-110.
5.
Nomura E, Inoue M, Kurimura M. Chondral and osteochondral injuries associated with acute patellar dislocation.
Arthroscopy.
2003;19:717-721.
6.
Nietosvaara Y, Aalto K, Kallio PE. Acute patellar dislocation in children: incidence and associated osteochondral fractures.
J Pediatr Orthop.
1994;14:513-515.
7.
Dainer RD, Barrack RL, Buckley SL, Alexander AH. Arthroscopic treatment of acute patellar dislocations.
Arthroscopy.
1988;4:267-271.
8.
Desio SM, Burks RT, Bachus KN. Soft tissue restraints to lateral patellar translation in the human knee.
Am J Sports Med.
1998;26:59-65.
9.
Fithian DC, Paxton EW, Stone ML, et al. Epidemiology and natural history of acute patellar dislocation.
Am J Sports Med.
2004;32:1114-1121.
10.
Larsen E, Lauridsen F. Conservative treatment of patellar dislocations: influence of evident factors on the tendency to redislocation and the therapeutic result.
Clin Orthop Relat Res.
1982;171:131-136.
11.
Carter C, Wilkinson J. Persistent joint laxity and congenital dislocation of the hip.
J Bone Joint Surg.
1964;46B:40-45.
12.
Dandy DJ, Desai SS. The results of arthroscopic lateral release of the extensor mechanism for recurrent dislocation of the patella after 8 years.
Arthroscopy.
1994;10:540-545.
13.
Hall JE, Micheli LJ, McManama GB Jr. Semitendinosus tenodesis for recurrent subluxation or dislocation of the patella.
Clin Orthop Relat Res.
1979;144:31-35.
14.
McConnell J. The physical therapist’s approach to patellofemoral disorders.
Clin Sports Med.
2002;21:363-387.
















