Article
Image IQ: Irregular ECG
A 41-year-old man whose ECG shows an ST elevation with an upwardly convex descent to an inverted T wave in leads V1 and V2. Labs showed hyperkalemia. What's your diagnosis?


A 41-year-old man whose ECG shows an ST elevation with an upwardly convex descent to an inverted T wave in leads V1 and V2. Labs showed hyperkalemia. What's your diagnosis? (©VisualDx)
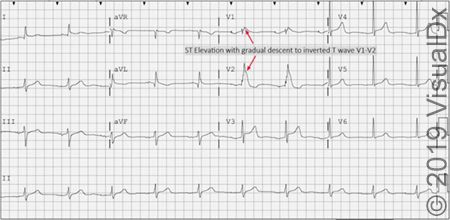
A 41-year-old man was rushed to the ED by EMTs after fainting while relaxing with his family in the evening. In the ambulance they recorded ventricular fibrillation and shocked his heart with a defibrillator to correct the rhythm. He was still experiencing heart palpitations and reported he had noticed them on and off in recent weeks. He was very upset because his father died suddenly of a heart attack in his early 40s and the man was worried he too would have a heart attack. His ECG showed ST elevation with an upwardly convex descent to an inverted T wave in leads V1 and V2, and labs showed hyperkalemia.
What's your diagnosis? For guidance, refer to the differential builder on VisualDx.
A. Long QT syndrome
B. Myocardial infarction
C. Brugada syndrome
D. Pulmonary embolism
See the next page for the answer.
ANSWER: C.) Brugada syndrome
Synopsis
The Brugada syndrome (BS) is characterized by ventricular arrhythmias in the presence of characteristic ECG abnormalities and a structurally normal heart, resulting in recurrent syncope and/or sudden cardiac death. It is usually genetically inherited in an autosomal dominant manner with incomplete penetrance. The underlying genetic defects generally cause reduced sodium inflow to cardiomyocytes during phase 0 of the cardiac action potential, thus shortening the duration of the action potential.
The initial presentation may be syncope or resuscitated sudden cardiac arrest due to polymorphic ventricular tachycardia or ventricular fibrillation. Onset is generally after adolescence, peaking in the third or fourth decade of life. Arrhythmias occur most commonly at night or at rest. The diagnosis may also be made on a routine ECG or family screening.
BS is reported to be responsible for 4% of all sudden deaths and 20% of sudden deaths in those without structural heart disease. A family history is present in about 20%-30% of patients. Prevalence in the general population is estimated at approximately 0.05%. It is particularly common among patients of Southeast Asian descent.
The "Brugada pattern" ECG consists of an atypical right bundle branch block with cove-shaped ST elevation in leads V1 to V3 in the absence of obvious structural heart disease, electrolyte disturbances, or ischemia. The ECG findings may be present at baseline or may only become apparent in the setting of a fever or with use of medications having sodium channel blocking activity, such as class I antiarrhythmics, tricyclic antidepressants, alcohol, or cocaine. Intermittent presence of the characteristic ECG pattern makes the diagnosis difficult in some patients.
For more information about this condition, incuding ICD 10 codes, visit VisualDx.
DISCLOSURE: This quiz was provided courtesy of VisualDx.

 in Cardiovascular Risk Assessment | Image Credit: UC Irvine")












