Article
Stress Fracture of the Base of the First Metatarsal Bone
Case study: Avid runner with midfoot pain: Stress fracture? Lisfranc ligament injury? Synovitis? The description of this rare fracture of the first metatarsal bone illustrates the importance of history and investigation.
ABSTRACT: A 29-year-old white man who is an avid runner presented with a 2½-year history of left midfoot pain on the dorsal area of the first metatarsal-cuneiform joint. Possible disorders included stress fracture of the base of the first metatarsal bone, Lisfranc ligament injury, extensor tendinopathy of the tibialis anterior tendon, synovitis of the metatarsal-cuneiform joint, and bone tumors. On the basis of the history and physical examination findings, stress fracture of the base of the first metatarsal bone was the diagnosis. The patient was placed in a foot and ankle brace for 6 to 8 weeks and received physiotherapy, forefoot strapping, and orthoses. The pain was alleviated significantly, and the patient resumed regular physical activity.
Leonardo da Vinci described the foot, an area of the lower extremities with a complex anatomy and biomechanics, as a “masterpiece of engineering.” However, forefoot injury often results from acute trauma or chronic overuse in athletes who participate in high-impact sports that involve running and jumping. The most common causes of forefoot pain in athletes are metatarsal stress fracture, sesamoid pathology, metatarsalgia, hallux valgus, and turf toe. A detailed history is vital in making a differential diagnosis and a diagnosis supported by investigations to provide a structured treatment plan.1,2
In this article, we present a rare case of stress fracture of the base of the first metatarsal bone in a young runner. The goal is to illustrate the importance of the history and investigations in the management of foot pain in athletes.
Presenting Complaint
A 29-year-old white man who is a writer and an avid runner presented to the clinic with a 2½-year history of left midfoot pain on the dorsal area of the first metatarsal-cuneiform joint. The main area of pain appeared to be over the medial dorsal area of the forefoot, around the base of the first metatarsal bone. There was some radiating pain over the first metatarsophalangeal (MTP) joint.
The patient described the pain as sharp and throbbing with variable intensity. It was rated between 0/10 and 8/10 on the Numeric Pain Scale. The pain sometimes disturbed sleep and caused the patient to have difficulty in going to sleep, although that varied with the patient’s activity level during the day. It was induced and increased with weight-bearing activities while the patient walked, ran, and jumped. He experienced some pain relief with rest, and the duration was variable. He sometimes felt numbness around the medial dorsal surface of the midfoot and forefoot.
History of Present Complaint
The pain originally occurred while the patient was running on a treadmill 2½ years earlier. There was no obvious history of acute trauma or injury to the left foot. The pain had a gradual onset and worsened with continued running. The patient felt a severe, sharp, shooting pain. At first, it was not localized, but it worsened after about 5 minutes of walking. After a variable period of rest, the pain would decrease in intensity but became a more diffused, dull, aching pain over the whole medial dorsal surface of the left foot.
There was no bruising, swelling, skin discoloration, skin lesion, temperature change, or obvious deformity, although the patient felt stiffness in his midfoot joints, with some limitation in the first MTP joint. He denied any previous injury to the left foot. The findings were largely unremarkable, with no significant history of musculoskeletal disease.
The patient kept fit by playing tennis on a regular basis and running about 10 to 15 miles per week, primarily on a treadmill but also on roads and cross-country. He stopped all his physical activity because of limitations imposed by his left foot pain.
The patient currently was using over-the-counter NSAIDs, which helped marginally. He received an injection of corticosteroids and anesthetic in the painful area, but there was no result. He has no drug allergy. He reported feeling well and fit.
Possible disorders in the differential diagnosis include the following:
• Stress fracture of the base of the first metatarsal bone
• Lisfranc ligament injury
• Extensor tendinopathy of the tibialis anterior tendon
• Synovitis of the metatarsal-cuneiform joint
• Bone tumors
Physical Examination Findings
Findings from the physical examination included the following:
• Observation. There was no swelling, redness, skin discoloration, scar tissue, or deformity in the hindfoot, midfoot, and forefoot sections of the patient’s left foot.
• Active movements. These were largely unremarkable. The patient could dorsiflex, plantar flex, evert, and invert the left foot without discomfort, pain, or limitation. He was able to flex and extend his digits with no obvious pain or discomfort.
• Passive movements. Flexion, extension, inversion, and eversion of the left foot were unremarkable; there was no obvious pain or discomfort. The patient’s first MTP joint movement was neither restricted nor painful.
• Resistive movements. There was discomfort and apprehension with resisted left foot movement in all planes. The patient felt specific acute pain at the metatarsal-cuneiform joint on plantar flexion and dorsiflexion of the first ray.
• Palpation. There was tenderness on the dorsal surface of the first metatarsal-cuneiform joint and noticeably more tenderness at the base of the first metatarsal in the left foot. There was no obvious tenderness over the sesamoid-metatarsal complex, MTP joint, interphalangeal joint, or intermetatarsal space. There were no plantar warts, calluses, or corns and no onychocryptosis. Tinel test results were negative. No abnormality other than analgesic gait was observed.
Discussion
• Stress fracture of the base of the first metatarsal bone. On the basis of the history and physical examination findings, stress fracture of the base of the first metatarsal bone-one of the most common causes of forefoot pain3-is the most likely diagnosis. In the forefoot region, the first and second metatarsal heads receive the greatest amount of energy transfer. A runner may absorb 110 tons per foot while running 1 mile.4 Pressure studies have shown that runners are weighted over the forefoot most of the time they are running.
The presence of focal tenderness in the forefoot area could suggest stress fracture. The pain is aggravated by walking and running and alleviated by rest.
Although first metatarsal stress fracture is rare, it should be included in the differential diagnosis when the patient complains of pain in the area of the first metatarsal bone after the forefoot trauma of repetitive use.5-7 Our clinical impression of this patient strongly suggests this diagnosis. The paresthesia and numbness of skin around the affected area could be the result of compression or irritation of the dorsal medial cutaneous nerve, which passes over the first metatarsal joint.
• Lisfranc ligament injury. Another possible cause of this patient’s pain is injury to the first metatarsal-cuneiform ligament. This injury varies from relatively minor to a fracture-dislocation. Instability or disruption of normal support may lead to significant pain and disability. The reported incidence of this uncommon injury is about 1 per 55,000 persons per year.8
The result is damage to the tight ligamentous structure of this joint complex, which creates an unstable foot for weight bearing. Chronic sprains, which may result from somewhat minor trauma, may be the most debilitating ones because of the pain experienced with weight bearing.
On physical examination, palpation elicits pain along the first metatarsal-cuneiform articulation; force applied to this area may elicit medial or lateral pain.9,10 Although the pain is localized around the first metatarsal head, injuries to this ligament could mimic such clinical impressions. More investigations should be performed to evaluate the first metatarsal-cuneiform joint.
• Extensor tendinopathy. Patients who have extensor tendinopathy usually complain of pain and discomfort at the insertion of the tibialis anterior tendon at the base of the first metatarsal-cuneiform joint after a period of vigorous exercise.3 Our patient experienced pain in the area of the tibialis anterior tendon insertion during resistant movements.
MRI has proved useful in detecting the various soft tissue, bone, and joint injuries and allows for specific diagnosis.11 In this patient, MRI could help make a diagnosis of extensor tendinopathy.
• Synovitis of the first metatarsal-cuneiform joint. Although this disorder is less common, it may be the cause of chronic forefoot pain in this patient.3 Further investigation should be done with MRI to evaluate for any synovial lesions in this joint.11
• Bone tumors. Another possible cause of pain, bone tumors, should not be missed during investigation. Bone tumors are rare in the forefoot, but they should be investigated in cases with prolonged foot pain in which they may be suspected.1,12
There are many reports of osteoid osteoma, but its occurrence in metatarsal bones is quite rare. This problem is more common in men than in women. The main clinical characteristic is mild dull pain relieved by aspirin. Pain sometimes worsens at night. The clinical picture and radiological findings often are atypical, possibly leading to misdiagnosis or delayed treatment after several months or years. Because the radiographic features of an osteoid osteoma often mimic stress fracture, this problem should be included in the differential diagnosis, especially in athletes who have prolonged forefoot pain and night pain.1,13
Further Investigation
A missed diagnosis of metatarsal stress fracture during a prolonged evaluation may result in complications of bone healing. These complications may include disability, delayed union, malunion, secondary osteoarthritis, and complex regional pain syndrome.
FIGURE 1



In this plain x-ray film of the patient’s left foot, no lesion is obvious.
A diagnosis of stress fracture may be confirmed by plain x-ray films, but not in the early stages of disease in 50% of cases.14 Therefore, the next step is bone scanning,3 which is not specific for stress fracture because a hot spot may be seen in fractures, degenerative changes, or neoplasms. In this patient, x-ray films did not show any significant changes or deformities (Figure 1). A bone scan revealed the solitary focal uptake near the base of the first metatarsal, suggesting stress fracture or tumor (Figure 2).
FIGURE 2


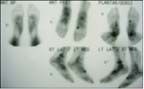
This bone scan shows a solitary focal uptake toward the base of the patient's left first metatarsal bone.
The patient received treatment, but the pain was not relieved. The next step could be MRI or CT to find what is causing the chronic pain. Possible causes include Lisfranc ligament injury, tibialis anterior tendinopathy, and bone tumor.
MRI scans of the patient’s left foot showed the focal area of bone marrow edema at the base of the first metatarsal bone and about the first metatarsal-cuneiform joint (Figures 3 and 4). Because the joint is not involved, an osteoid osteoma may have been indicated. In this MRI scan, no definite fracture line was reported. The rest of the foot was described as normal.
FIGURE 3


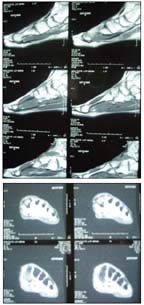
A T1-weighted MRI scan shows focal edema at the base of the patient’s first metatarsal bone of the left foot.
For making a clear diagnosis, CT should be performed for better assessment of the bony lesion. Because a diagnosis of osteoid osteoma may be difficult in complex anatomical sites, CT remains the modality of choice for diagnosis and precise localization of this tumor and intra-articular lesions. MRI findings are extremely variable and generally nonspecific.15-17 If a CT scan reveals osteoid osteoma, the major treatment is resection of tumor and radiographic evaluation of the patient.12,17
To look for anatomical instability in assessment of Lisfranc ligament injury, plain x-ray films in the standing position, the full weight-bearing position on the affected foot, or stress views are recommended. If the x-ray film finding is normal, further investigation, such as MRI, should be performed. If MRI is unavailable, bone scanning is suggested. If bone scan findings are positive, CT also should be performed.
FIGURE 4



A short-tau inversion-recovery MRI scan of the patient’s left foot shows positive signal in the base of the first metatarsal bone.
The proper treatment for a patient with a mild to moderate Lisfranc injury improves the chances of successful healing and reduces the chances of complications. Patients with fractures or fracture-dislocations should be referred for surgical management.3,9
Treatment
The patient was reviewed by a multidisciplinary team. After further evaluation, stress fracture was the diagnosis. The patient was placed in a foot and ankle brace for 6 to 8 weeks and received physiotherapy, forefoot strapping with a well-molded arch support, and orthoses. The pain was alleviated significantly. After 8 weeks of treatment, the patient resumed regular physical activity.
References:
REFERENCES
1. Sakamoto K, Mizuta H, Okajima K, Kitagawa T. An unusual cause of metatarsal pain in a young kendo player. Am J Sports Med. 1989;17:296-297.
2. Lillich JS, Baxter DE. Common forefoot problems in runners. Foot Ankle. 1986;7:145-151.
3. Brukner P, Khan K, Agosta J. Foot pain. In: Brukner P, Khan K, eds. Brukner & Khan’s Clinical Sports Medicine. 2nd rev ed. Sydney, Australia: McGraw-Hill Australia; 2001:584-601.
4. The foot: endurance events, marathon. In: Safran MR, McKeag DB, Van Camp SP, eds. Manual of Sports Medicine. Philadelphia: Lippincott-Raven; 1998:485, 558-559.
5. Coughlin MJ. Common causes of pain in the forefoot in adults. J Bone Joint Surg. 2000;82B:781-790.
6. Hockenbury RT. Forefoot problems in athletes. Med Sci Sports Exerc. 1999;31(7 suppl):S448-S458.
7. Lucas MJ, Baxter DE. Stress fracture of the first metatarsal. Foot Ankle Int. 1997;18:373-374.
8. Kaplan JD, Karlin JM, Scurran BL, Daly N. Lisfranc’s fracture-dislocation: a review of the literature and case reports. J Am Podiatr Med Assoc. 1991;81:531-539.
9. Burroughs KE, Reimer CD, Fields KB. Lisfranc injury of the foot: a commonly missed diagnosis. Am Fam Physician. 1998;58:118-124.
10. Shapiro MS, Wascher DC, Finerman GA. Rupture of Lisfranc’s ligament in athletes. Am J Sports Med. 1994;22:687-691.
11. Ashman CJ, Klecker RJ, Yu JS. Forefoot pain involving the metatarsal region: differential diagnosis with MR imaging. Radiographics. 2001;21:1425-1440.
12. Hoeffel JC, Segal P, Abadou H, Adnet JJ. Osteoblastoma of the first metatarsal bone. Rofo. 1989;151:506-507.
13. Georgoulis AD, Soucacos PN, Beris AE, Xenakis TA. Osteoid osteoma in the differential diagnosis of persistent joint pain. Knee Surg Sports Traumatol Arthrosc. 1995;3:125-128.
14. Courtenay BG, Bowers DM. Stress fractures: clinical features and investigation. Med J Aust. 1990;153:155-156.
15. Hachem K. Haddad S, Aoun N, et al. MRI in the diagnosis of osteoid osteoma [in French]. J Radiol. 1997;78:635-641.
16. Orzincolo C, Cerutis S, Cardona P, et al. Diagnostic imaging of osteoid osteoma [in Italian]. Radiol Med. 1996;92:351-357.
17. Röderer G, Nelitz M, Puhl W, Huch K. Minimally invasive therapy for osteoid osteoma [in German].
Z Orthop Ihre Grenzgeb. 2004;142:456-461.
















