News
Article
After Elevidys: DMD Advocacy Past First Gene Therapy Approval
Author(s):
For This Year in Medicine, CGTLive looks back at a landmark first approval, the new treatment opportunities it has provided, and the unmet needs in the field it has brought to light.
Although the road has not been smooth, 2023 was witness to unprecedented progress in the treatment landscape of Duchenne muscular dystrophy (DMD), with the approval of Sarepta Therapeutics’ delandistrogene moxeparvovec (SRP-9001; Elevidys) earlier this summer.1 Despite the milestone approval, only a small percentage of patients with DMD currently stand to benefit from the therapy. There is much work to be done in the field to improve care for all patients with DMD as well as to answer questions about the gene therapy’s long-term durability, efficacy, and safety.



Elevidys is an adeno-associated virus (AAVrh74) gene therapy delivering microdystrophin. It was approved for ambulatory pediatric patients aged 4 through 5 years with a confirmed mutation in the DMD gene, excluding patients with any deletion in exon 8 and/or exon 9. Its approval was based on data from Study 102 (NCT03769116), Study 103 (ENDEAVOR; NCT04626674), and Study 101 (NCT03375164). Study 102 failed its primary North Star Ambulatory Assessment (NSAA) end point although subgroup analyses revealed the strongest clinical benefit in boys aged 4-5 years, supporting the approval in only that narrow population.
“There's still significant unmet need. While the gene therapy approval is thrilling for all of us, there's still a narrow window of 4- to 5- year-olds. We have many people younger than 4 and many people over the age of 5, that are still in need of treatment. So, I think while the landscape is really amazing, and building every single day... time matters to these people. Time means progression of disease,” Pat Furlong, BSN, RN, founding president and chief executive officer, Parent Project Muscular Dystrophy (PPMD), told CGTLive.



Sarepta recently announced topline data from its global, pivotal, phase 3 EMBARK study (Study SRP-9001-301; NCT05096221), which was also found to have failed its NSAA primary endpoint. The EMBARK study’s key primary end point was change in scores at week 52 compared to placebo, the difference in which was not statistically significant. Treated patients improved 2.6 points on NSAA total score compared to 1.9 points in placebo-treated patients for a 0.65-point difference (n = 125; P = .24). Key secondary end points of change in time to rise (TTR; P = .0177) and 10-meter walk test (10MWT; P = .0048) compared to placebo were statistically significant across all age groups. Although the complete data are not yet available, Sarepta also stated that other outcome measures such as stride velocity 95th centile (SV95C) and time to ascend 4 steps also demonstrated a consistent trend in treatment benefit in favor of ELEVIDYS.2
“This drug is likely to be the most potent treatment method available today, although it is not as robust as many had hoped. Nonetheless, approval sets the stage for intensive analysis of the long-term effects of this gene therapy and will hopefully spur increased research and testing of improved next generation gene therapies," Jeffrey Chamberlain, PhD, professor and director, Sen. Paul D. Wellstone Muscular Dystrophy Specialized Research Center, University of Washington School of Medicine told CGTLive.
The data have somewhat dampened the enthusiasm of many patients and advocates that were hoping the gene therapy might be a permanent, revolutionary treatment for DMD. The data are current only available from 12 months of follow-up, and it remains to be seen how many years of durability current gene therapies will really yield—for both DMD and all fields with recent approvals of this relatively new mode of therapy.
“Some of the concerns that we have today are with these very high dose serious adverse events, that's one of the challenges with Duchenne. When you think that the body is comprised of 40 to 60% muscle – the amount of AAV that we need to put in the body in order to target all the different muscle groups is extremely high... Changing the actual route of administration may hold significant promise. And it's these data that are going to guide some of our thinking next year beyond where we are today,” Michael Kelly, PhD, chief scientific officer of CureDuchenne, told CGTLive.
As dystrophin is the largest known human gene, the carrying capacity of AAV limits the feasibility of gene therapy to correct the mutated gene. Most companies including Sarepta have instead designed their gene therapies to express microdystrophin instead, but future research and new mechanisms of action and delivery may show greater efficacy and safety. Part of the difficulty in showing a definitive benefit with gene therapy is the heterogeneity of disease seen in patients with DMD and advocates are also pushing for the design of more accurate and precise outcome measures.
“We don't see the full effect in that time period of clinical trials. We have to look for extended access programs, or certainly the cumulative data over time, to see both the durability and efficacy of these cell and gene therapies. I’m very thrilled about where we are, and hopeful for where we're going next,” Furlong said.
The criteria of Elevidys’ approval exclude most patients with DMD, including patients aged 6 - 7 years that were included in the pivotal trials of the therapy. Sarepta is continuing to work toward expanding the therapy’s approval to include older children and has cited the statistically significant changes in EMBARK’s secondary endpoints, seen across children aged both 4 - 5 years old and 6 - 7 years old, as support for an expanded approval. It remains to be seen whether further data from the study will support the move. Regardless of gene therapy’s potential future expansion to older patients, the treatment landscape for DMD in general must expand to provide care to patients that may not qualify for the newest, novel therapies.
Besides age, anti-AAV antibodies (nAB) remain a barrier gene therapy, whether patients are nAB+ from wild-type infections or prior AAV gene therapy. The latter becomes more of a concern as more AAV gene therapies are approved or enter the investigational pipeline with no current means of suppressing nABs, preventing patients from receiving other, possibly more efficacious, gene therapies in the future.
“Is there a window in which we need to treat early and is there some way we can manage people who have progressed past that window instead of just saying, well, they're not eligible for these drugs? What can we do for them? It may be a really different strategy. With gene therapy, where you're putting back the function of this gene that's missing, you can't put it into muscle that's not there. I think that's where we should be looking at combinations of things like stem cell therapy or other creative ways where we could potentially replace muscle. So, I think we're going to have to develop some new strategies for people who progress past that therapeutic window,” Sharon Hesterlee, PhD, chief research officer, Muscular Dystrophy Association (MDA), told CGTLive.


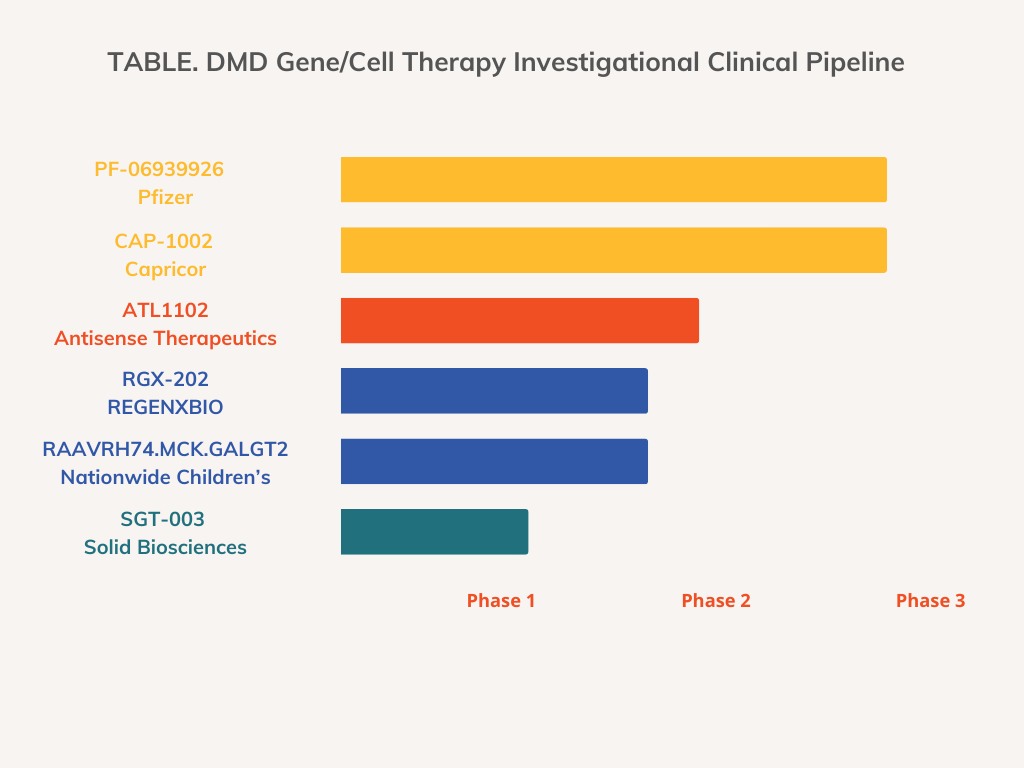
Experts and advocates in the field continue to stress that this first-of-its-kind approval is a first step to potentially curing DMD and future research will continue to build off of lessons learned with Elevidys. Other programs far along the pipeline for treating DMD include Capricor Therapeutics’ CAP-1002, an investigational allogeneic cardiosphere-derived cell therapy being evaluated in the HOPE-3 clinical trial (NCT05126758); REGENXBIO’s AAV gene therapy RGX-202 being evaluated in the phase 1/2 AFFINITY trial (NCT05693142); and Pfizer’s fordadistrogene movaparvovec AAV gene therapy being evaluated in the phase 3 CIFFREO trial (NCT04281485).3,4
“I think we're going to have enough variety of options that everyone is going to have the potential to benefit. I think it's very exciting. The big challenge for us as a community is figuring out how do we make that work... Every step forward brings new obstacles, but you're still making progress," Hesterlee said.
References
- Sarepta Therapeutics Announces FDA Approval of ELEVIDYS, the First Gene Therapy to Treat Duchenne Muscular Dystrophy. News release. Sarepta Therapeutics. June 22, 2023. News release. Sarepta Therapeutics. June 22, 2023. https://investorrelations.sarepta.com/news-releases/news-release-details/sarepta-therapeutics-announces-fda-approval-elevidys-first-gene
- Sarepta Therapeutics announces topline results from EMBARK, a global pivotal study of ELEVIDYS gene therapy for Duchenne muscular dystrophy. News release. Sarepta Therapeutics. October 30, 2023. https://investorrelations.sarepta.com/news-releases/news-release-details/sarepta-therapeutics-announces-topline-results-embark-global-0
- Capricor Therapeutics announces positive Type-B meeting with the FDA to discuss pathway to BLA for CAP-1002 in Duchenne muscular dystrophy. News release. Capricor Therapeutics. September 29, 2023. Accessed October 3, 2023. https://www.capricor.com/investors/news-events/press-releases/detail/261/capricor-therapeutics-announces-positive-type-b-meeting
- REGENXBIO presents interim clinical data from phase I/II AFFINITY DUCHENNE™ trial of RGX-202 at 28th Annual International Congress of the World Muscle Society. News release. REGENXBIO. October 3, 2023. https://www.prnewswire.com/news-releases/regenxbio-presents-interim-clinical-data-from-phase-iii-affinity-duchenne-trial-of-rgx-202-at-28th-annual-international-congress-of-the-world-muscle-society-301946289.html














