Publication
Article
Family Practice Recertification
A Heart Swings Sadly to a Diagnosis
Author(s):
A 47 year old woman with no past medical history presented with back pain a month prior, and an MRI of the lumbar spine was performed and demonstrated a mass protruding into S1 concerning for hemangioma.
A Heart Swings Sadly to a Diagnosis
A 47 year old woman with no past medical history presented with back pain a month prior, and an MRI of the lumbar spine was performed and demonstrated a mass protruding into S1 concerning for hemangioma.
She now presents with 2 weeks of increasing shortness of breath and cough. She denies chest pain, palpitations or light-headedness. She is a thin woman appearing her stated age in mild respiratory distress with movement. Her heart rate is 130 bpm. Blood pressure is 100/50. Breath sounds are diminished at the right posterior lung base and a cardiac exam is notable for tachycardia but also a regular rhythm with no murmurs or rubs. A pulse oximeter is placed and she has an oxygen saturation of 92% on room air. An EKG is performed.


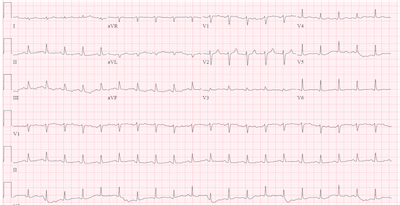
The EKG reveals a regular narrow complex tachycardia with upright P waves preceding every QRS consistent with a sinus tachycardia. The QRS complexes are notably low voltage for a thin, young woman. Low voltage is most specifically diagnosed when the QRS amplitude is less than 5 mm in the limb leads and less than 10 mm in the precordial leads. Despite her having 6-6 mm of amplitude in the inferior leads (II, III and aVF), I would read this as low voltage.
Voltage can be low when there is loss of myocardial tissue (e.g. myocardial infarction), increased tissue, air or fluid between the heart and the electrodes (e.g. emphysemia, effusions) or with infiltration of cardiac tissues (e.g. amyloid, hemachromatosis). The rhythm strips have an undulating appearance which is in part due to her respirations, but a close look at some of the leads, especially II and V4, reveal amplitude that changes in magnitude every other QRS. The first, third and fifth beat of V4 are 7 mm while the second and fourth beats are only 3 mm in amplitude. This is consistent with electrical alternans. Electrical alternans is a change in amplitude and/or direction of the QRS every other beat. Electrical alternans can be seen with severe left ventricular failure, deep inspirations and coronary artery disease.
The combination of low voltage and electrical alternans is suggestive but not diagnostic of a pericardial effusion or tamponade, but would be particularly suggestive in the setting of shortness of breath, tachycardia and low blood pressure.
At the bedside, checking for a change in the systolic blood pressure of greater than 10 mm Hg with inspiration is consistent with cardiac tamponade. It may be possible to feel a drop in amplitude of the radial pulse with inspiration. Because the fluid around the heart impairs filling of the heart, the jugular venous pressure will be elevated and jugular veins will be distended. Lastly, the cardiac sounds may be muffled due to the insulating effects of fluid around the heart. The triad of muffled cardiac sounds, distended neck veins and low blood pressure is pathognomonic for acute cardiac tamponade but is present in a minority of cases.
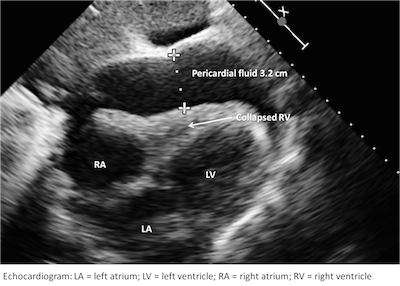
The patient was sent to the emergency department where a stat echocardiogram and CT chest were performed. The CT demonstrated a 7 cm mass in the right hilar space. The echo confirmed a very large pericardial effusion with tamponade physiology by Doppler exam.


The relative absence of shock should not sway from immediate cardiology consultation. Although the effusion may have slowly accumulated allowing her to compensate for a time, her worsening symptoms shock index (HR>SBP) should prompt immediate consultation before she decompensates. An emergent pericardiocentesis was performed draining 650 mL of bloody fluid with normalization of her hemodynamics and improvement in her respiratory status. Fluid was sent for analysis and was positive for lung adenocarcinoma (TTF1 and Napsin A positive) with molecular markers negative for EGFR, ALK and KRAS. Oncology was consulted and the patient is receiving treatment as an outpatient for metastatic non-small cell lung cancer, adenocarcinoma with good treatment response.
Jabob S, Sebastian J, Cherian P, Abraham A, John S. Pericardial effusion impending tamponade: a look beyond Beck’s triad. Am J Emerg Med. 2009;27:216-219
Bilchick KC, Wise RA. Paradoxical physical findings described by Kussmaul: pulsus paradoxus and Kussmaul’s sign. Lancet. 2002;359:1940-1942




 in Cardiovascular Risk Assessment | Image Credit: UC Irvine")










