Publication
Article
Family Practice Recertification
An Infant Who Swallowed a Coin
Author(s):
A mother brought her 1-year-old daughter to the emergency department and reported that the child had swallowed a coin. She had vomited once without recovery of the coin. The mother said the baby had not been coughing or wheezing and had no respiratory distress, but she refused to eat.
CINICAL HISTORY
A mother brought her 1-year-old daughter to the emergency department and reported that the child had swallowed a coin. She had vomited once without recovery of the coin. The mother said the baby had not been coughing or wheezing and had no respiratory distress, but she refused to eat.
An anterior posterior radiograph of the neck and thorax (Figure 1) and a lateral radiograph of the head and neck (Figure 2) revealed a coin at the lower cervical level of the esophagus. A chest radiograph (not displayed) and an anterior posterior radiograph of the abdomen (Figure 3) displaying the coin had advanced into the stomach.
Before radiography, the differential diagnosis included a foreign body in the esophagus and a foreign body in the airway. After the radiographic studies, laryngoscopy and esophagoscopy were performed under general anesthesia in the operating room and confirmed the coin was in the esophagus and not in the trachea.
Discussion
The ingestion of foreign bodies is most commonly a problem in young children aged 6 months to 5 years. The event is often witnessed by parents as in the case of this patient. Objects commonly ingested by children include coins, small toys, pencils, pens and their tops, batteries, safety pins, needles and hairpins.
The majority of ingested foreign bodies will pass safely through the gastrointinal tract and be passed with feces. Patients swallowing foreign bodies are usually asymptomatic but may have difficulty in eating.
A leading cause of emergency admissions for infants and children is foreign body aspiration or swallowing. The foreign body may lodge in the three narrowed sites of
the esophagus: below the cricopharyngeal muscle at the arch of the aorta, at the hiatus
of the diaphragm, and at the cardia. Congenital and developmental strictures may also be responsible for trapping foreign bodies.
The initial symptoms may include gagging, choking, and coughing. If the object is left in place, localized pain can develop at the thyroid cartilage along with drooling and difficulty swallowing. If the object becomes fixed, edema develops, and infection with
perforation that may follow.
A parent may see the child swallow the object and make the initial diagnosis. If the object appears dis-coid on a radiograph as it did in this patient, it will occupy the coronal plane and can be easily distinguished from an object in the trachea. Fluoroscopic examination of the neck, chest, and abdomen may locate the object documented by radiographic imaging as in this case.
A foreign body in the esophagus requires immediate attention. Esophagoscopy can be performed to locate and remove the object without complication. Urgent removal is of particular importance for sharp objects as well as for disk batteries.
Foreign bodies in the alimentary tract distal to the esophagus will usually pass unless they have an unusual shape or sharp margin larger than 3.5 cm (the limiting size for passage beyond the ligament of Treitz). Surgical removal may be required. The rule is any radiological evidence of a stationary foreign body beyond the pylorus for 5 days indicates obstruction.
In this case, the metal object was passed through the alimentary tract without further complications.
Take-home message
When an infant or child swallows an object and it is not immediately recovered, parents should seek immediate medical attention. Documentation by permanent neck, chest and abdominal radiographs should be mandatory before any invasive studies are requested.
Should the foreign body not be dense enough to be visualized, oral water soluble contrast may be necessary to identify the object.
Food and liquid intake should be withheld until the child is medically released to avoid aspiration. Radiographs of the neck, chest and abdomen should also be obtained following removable of foreign bodies for baseline follow-up information.
Figure Legends


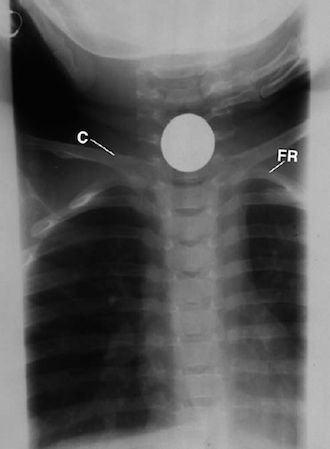
Figure 1 This anterior posterior (AP) cone-down radiograph of the neck and thorax
displays the metal coin in the coronal plane over the mid region of the lower neck at the thoracic inlet. C = clavicle, FR = left first rib of the thoracic spine.



Figure 2 This is a left lateral radiograph in the sagittal plane of the head and neck displaying the metal coin over the region of the esophagus within the anterior lower cervical spine. No significant edema is demonstrated. C = coin, E = earring, EP = epiglottis, H = hyoid bone, T = tongue, TR = trachea, 5 = 5th cervical vertebra.



Figure 3 This anterior posterior radiograph of the abdomen displays
the metal coin over the region of the atrium of the stomach.
DP = diaper pin, S = stomach.
















