Publication
Article
Family Practice Recertification
Determining the Proper Servings of Fruits and Vegetables
Author(s):
This study was designed to determine the dose-response relation between fruit and vegetable consumption and risk of all cause, cardiovascular, and cancer mortality.



Frank J. Domino, MD
Review
Wang, Xia, et al. “Fruits and Vegetables Win Again.” BMJ 2014; 349:g4490.
This study was designed to determine the dose-response relation between fruit and vegetable consumption and risk of all cause, cardiovascular, and cancer mortality.
Study Methods
Meta-analysis of cohort studies including over 800,000 adult patients where fruit and vegetable consumption was followed and reported outcomes, particularly, deaths. From the initial 7,000 articles found, 16 were included that demonstrated 56,423 deaths (11,512 from cardiovascular disease and 16,817 from cancer).
Results and Outcomes
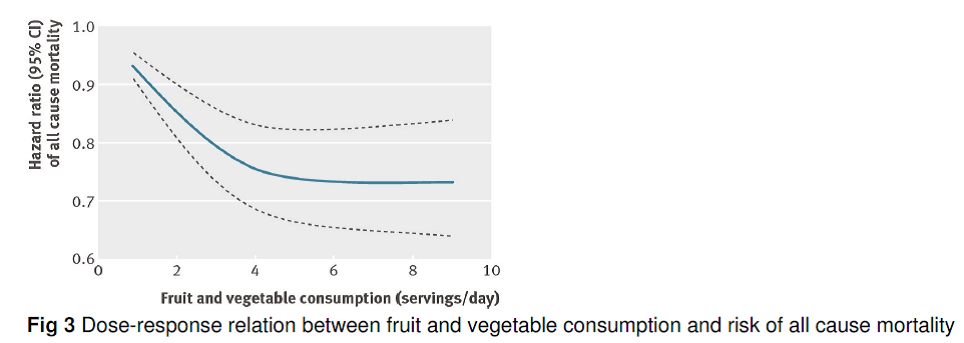
Regarding all cause mortality, higher fruit and vegetable consumption was associated with lower risk. The pooled hazard ratios for all cause mortality were 0.95% for each increment of one serving of fruits and vegetables per day. The optimal benefit was seen at 5 servings of fruits and vegetables a day; greater consumption did not alter the risk of all cause mortality. This inverse association was also associated with cardiovascular mortality.
Compared with no daily consumption of fruits and vegetables, the estimated hazard ratio of all cause mortality was 0.92% for one serving per day, 0.85% for 2 servings per day, 0.79% for 3 servings a day, 0.76% for 4 servings a day, 0.74% for 5 servings per day, and 0.74% for 6 or more servings per day. For cardiovascular mortality in particular, each additional serving per day of fruits and vegetables reduced cardiovascular mortality by 4%, with a slightly increased benefit when more fruits than vegetables were consumed.
Conclusion
Eating 5 servings of fruits and vegetables per day had the greatest impact on lowering all-cause, cardiovascular, and cancer-related mortality. The ideal combination found by this study was 2 servings of fruit and 3 servings of vegetables per day. On close examination, the average reduction of 5% was found for each additional serving of fruit and vegetable on all cause mortality. This was most prominent for cardiovascular mortality, but was less so for cancer mortality.
Commentary
Western medicine has long chased after a single pill or even a combination of pills (polypill) to provide optimal cardiovascular and cancer mortally reduction. Cardiovascular disease continues to be the leading cause of death among US citizens, followed closely by cancer mortality. Finding a single treatment modality to address both of these issues would have a huge impact on life expectancy.
We have found that solution. It does not come from a prescription pad or a vitamin bottle. It comes from how we approach our dietary intake. There has been considerable data, especially pointing towards the Mediterranean diet, demonstrating benefit from increased degrees of fruits and vegetables on all cause mortality and cardiovascular disease. There have been specific cancer reductions, most prominent colorectal cancer, from higher levels of food based dietary fiber. While this study did not find an overall cancer reduction, there is still a strong body of data supporting benefit of fruit and vegetable intake on specific cancers.
The best way to incorporate this information into clinical practice is to ask patients at their health maintenance visit to perform a “24 Hour Dietary Recall.” That is, to verbally recount everything they ate the day before while you count the number of servings of fruits and vegetables they consumed. Although this study did not identify which vegetables and fruits were included, it would be important to exclude potatoes and white rice as vegetables due to their relatively low fiber and nutritional value.
Having been taught this by Jill Grimes, MD, from Austin, TX, many years ago, I have employed this technique and found many patients often eat one (or even no) fruits and vegetables every day. By encouraging 5 servings a day for patients, you will likely provide a greater all cause mortality benefit than any pill you can prescribe.
And for those patients who wish to lose weight, pushing this limit closer to 10 servings of fruits and vegetables per day will provide both cause a reduced mortality benefit as well as weight loss, and possibly diabetes prevention. Combine this study with a brief exercise plan (see other FPR JC article on leisure time running from the Journal of the American College of Cardiology 2014; 64(5):472-81) and you will be providing your patients with the absolute best disease prevention we can offer adults.
There are many theories as to why the United States is one of the most obese nations in the world. There are also a variety of theories that explain why we rank 42nd in the world in life expectancy compared to many other nations where healthcare expenditures are less by a factor of 3. This study may not explain that discrepancy in whole, but it likely explains a great deal about our personal habits. And far more than any medication or surgical intervention, can have an exceptional impact on our future health. ‘5 a day” should be a part of every adult visit!
About the Author
Frank J. Domino, MD, is Professor and Pre-Doctoral Education Director for the Department of Family Medicine and Community Health at the University of Massachusetts Medical School in Worcester, MA. Domino is Editor-in-Chief of the 5-Minute Clinical Consult series (Lippincott Williams & Wilkins).
Additionally, he is Co-Author and Editor of the Epocrates LAB database, and author and editor to the MedPearls smartphone app. He presents nationally for the American Academy of Family Medicine and serves as the Family Physician Representative to the Harvard Medical School’s Continuing Education Committee.





 in Cardiovascular Risk Assessment | Image Credit: UC Irvine")










