Publication
Article
Family Practice Recertification
Why Does This Patient Have a Hyperlucent Right Lung and Rib Deformities?
Author(s):
This is a 23-year-old female admitted for the first time who provides the history of congenital right chest wall deformity, right hypoplastic breast and absent right pectoralis muscles (1). Preliminary upright PA, lateral and right posterior oblique radiographs were obtained to evaluate the osseous and soft tissues of the thorax prior to cosmetic surgery and repair. No past history was made available.

James D. Collins, MD
History
This is a 23 year-old female admitted for the first time who provides the history of congenital right chest wall deformity, right hypoplastic breast and absent right pectoralis muscles (1). Preliminary upright PA, lateral and right posterior oblique radiographs were obtained to evaluate the osseous and soft tissues of the thorax prior to cosmetic surgery and repair. No past history was made available.
Radiographic Findings
FIGURE 1 is an upright PA chest radiograph that displays the anatomical distortion of the right second through fifth ribs; manubrium sloping right; hyperlucent right lung suggesting absence of the pectoralis muscles as per history given; elevated small right scapula compared to the left scapula; small right hemithorax as compared to the left; non-visualization of the right breast; right concave scoliosis of the thoracic spine, 1T-8T; absence of soft tissue fat over the right hemithorax.
Figure 2 is the left lateral upright chest radiograph that displays the backward displaced upper anterior right ribs (2-5) reflecting loss in tension at the insertion of the pectoralis muscles; asymmetric heads of the clavicles insertion on the manubrium, right lower than left; absence of the right breast; backward displacement of the inferior vena cava and left ventricle.
Figure 3 is the upright posterior oblique radiograph that displays the hyperlucent right lung and asymmetric right upper ribs as above describes in Figure 2; absence of the right serratus anterior muscles over the right ribs (1-3)


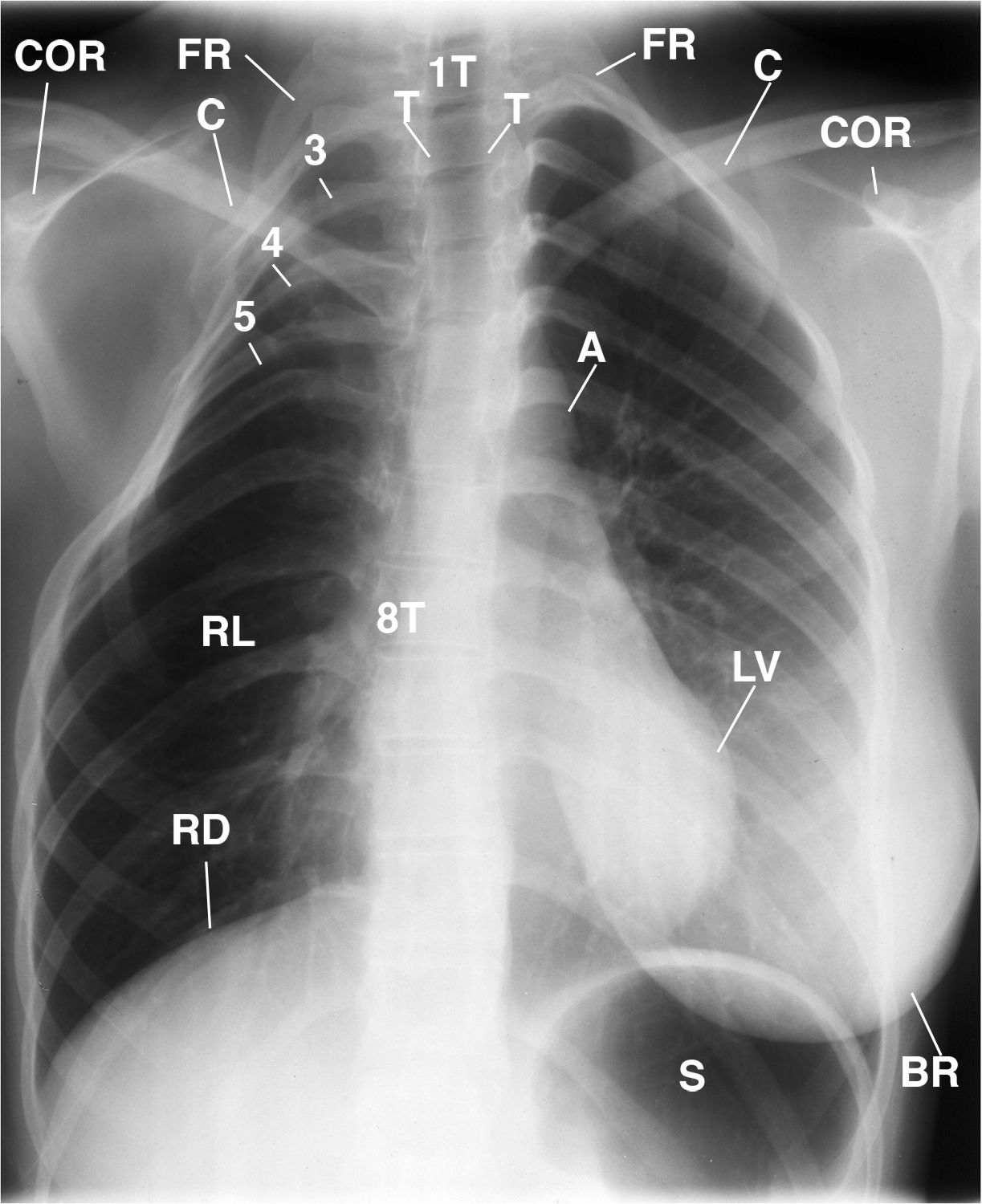
FIGURE 1. This image displays the smaller right scapula (not labeled) as compared to the left; right first rib (FR) and the upper ribs ( 3, 4, 5) and 6-9 (not labeled); hyperlucent right lung (RL); right concave scoliosis of the thoracic spine (1T-8T); forward left coracoid process (COR) as compared to the right, and the high left clavicle (C) compared to the right reflecting greater laxity of the sling/erector muscles on the right than left, Aorta (A), LEFT BREAST (BR), LEFT VENTRICLE (LV), RIGHT HEMIDIGRAM (RD). RIGHT LUNG (RL). STOMACH (S) TRACHEA (T).


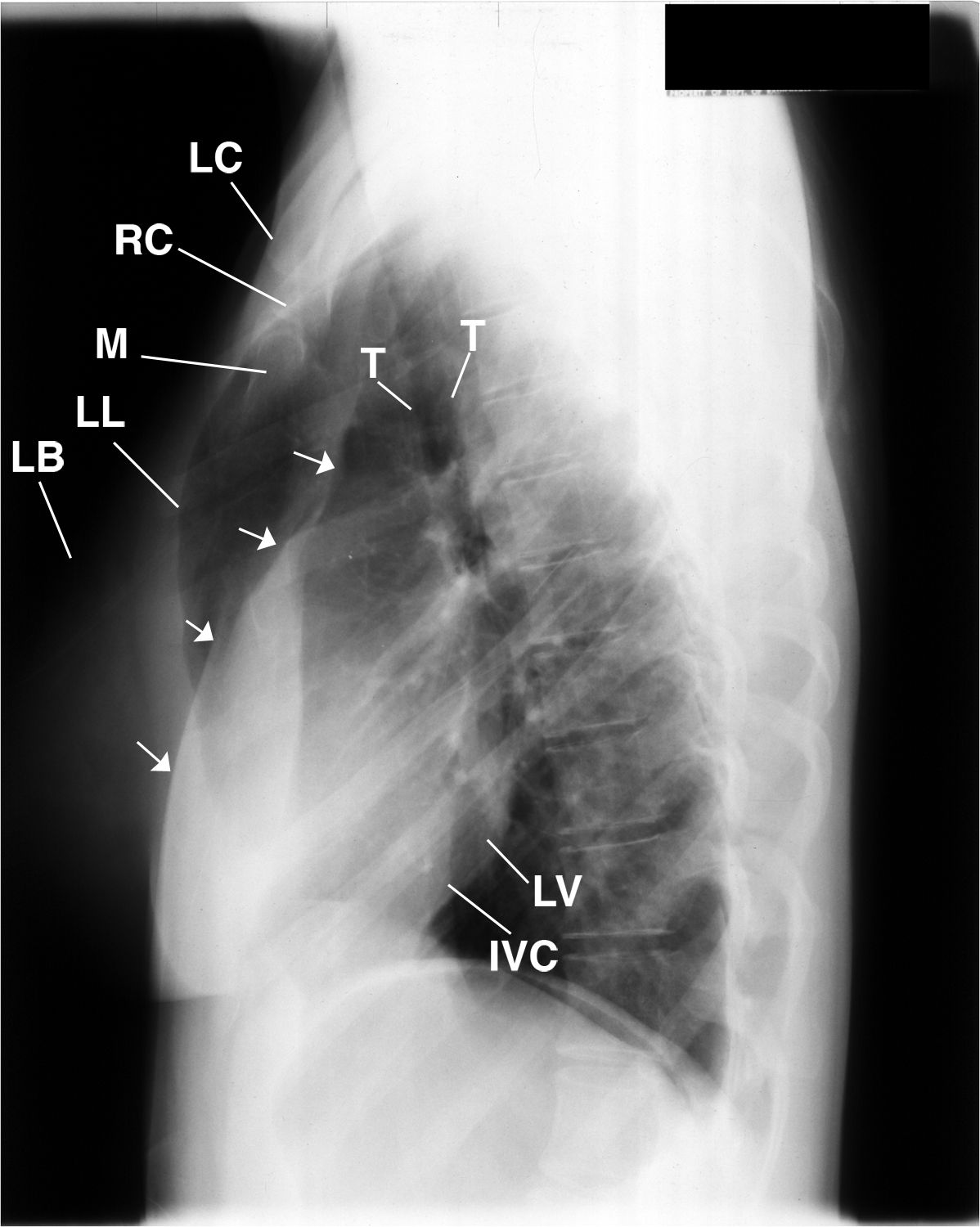
FIGURE 2. This is the lateral chest radiograh that cross references the PA above (FIGURE 1) image that displays the left breast (LB), pleura of the left lung (LL) and right lung (arrows), INFERIOR VEVA CAVA ( IVC), LEFT VENTRICLE (LV), MANUBRIUM (M), RIGT AND LEFT CLAVICLES (RC, LC); LEFT BREAST (LB), and the TRACHEA (T).


FIGURE 3. This is the right posterior oblique of FIGURE1 that displays the hyperlucent right lung (RL), neck of the small right scapula (S); deformed right first rib to the 5th right rib (FR-5), right side of the manubrium (not labeled) inferior to the right sixth rib (not labeled). RIGHT CLAVICLE (C), RIGHT HEMIDIAPHRAM (RD), HEAD OF THE RIGHT HUMERUS (H).


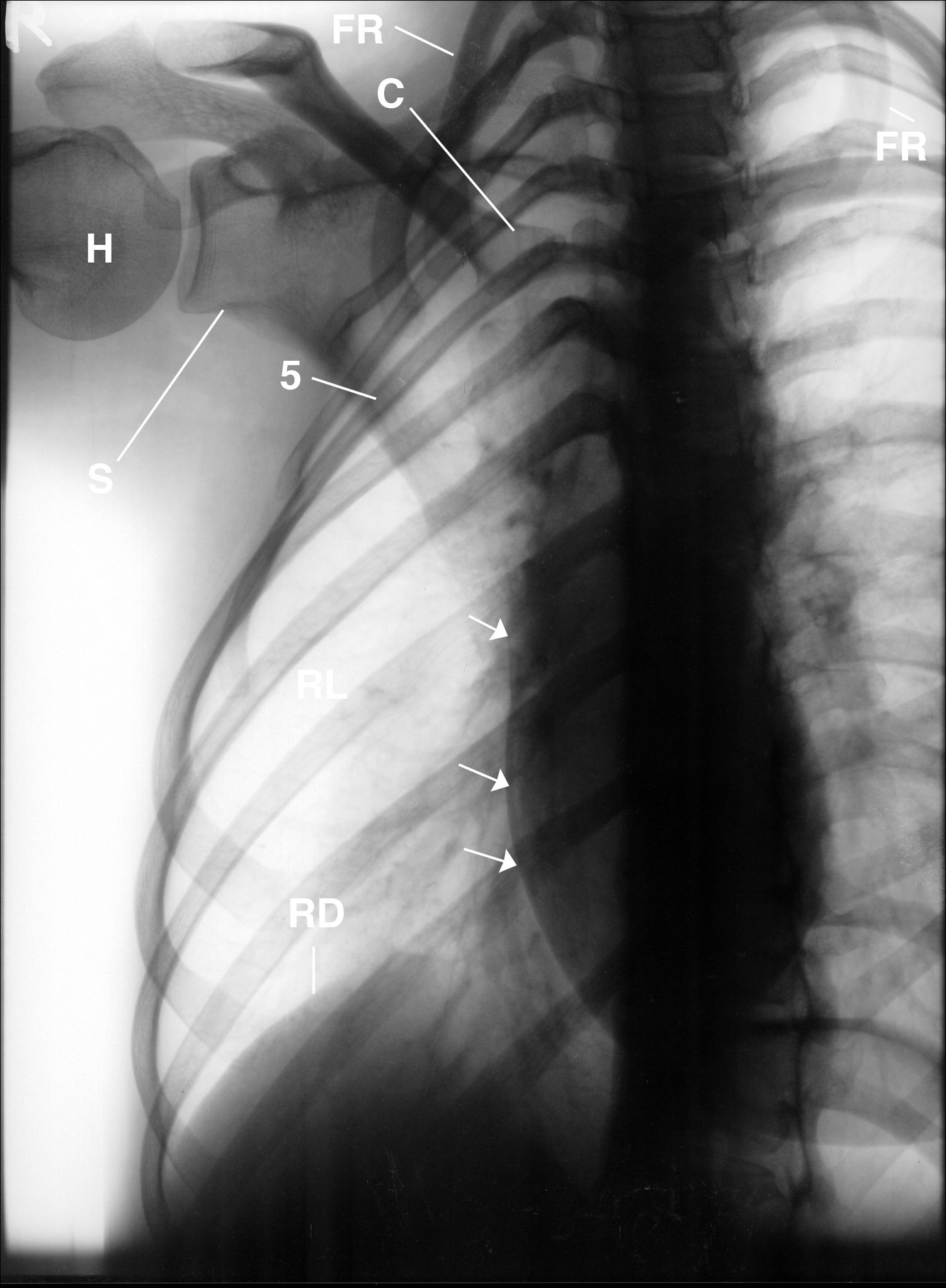
FIGURE 4. This is an inverted image of the right posterior oblique of FIGURE 3 that provides a different perspective accenting the hyperlucent right lung and the absence of fat over the right hemithorax. Three arrows marginate the left breast. hyperlucent right lung (RL), small right scapula (S), deformed right first rib to the 5th right rib (FR-5), RIGHT CLAVICLE (C), RIGHT HEMIDIAPHRAM (RD), HEAD OF THE RIGHT HUMERUS (H).
Diagnosis
1. Right chest wall deformity as described above.
2. Hyperlucent right lung.
3. Absent right breast.
4. Right concave scoliosis of the thoracic spine, 1T-8T.
5. Absent right serratus anterior muscles.
6. Small right hemithorax
Discussion
The patient provided the information that she had congenital right chest wall deformity, right hypoplastic breast and absent right pectoralis muscles, but no documents supported her presenting history. The congenital absence of the right breast, unilateral hyperlucent lung and absence of the pectoralis muscles on the chest radiographs suggested this would be a case of Poland’s syndrome.
Patients who have atrophy of chest wall muscles secondary to polio or disuse, post-surgical hypoplasia of the entire lung, mainstem bronchus obstruction by a foreign body, inflammatory disease or surgery, thrombotic emboli in the lungs, spontaneous pneumothorax and Sprengel’s deformity may also present with a unilateral hyperlucent lung.
Poland’s syndrome is an anatomic variation of the anatomy. It is an uncommon congenital anomaly characterized by unilateral anomalies of the chest wall and upper extremity. Males are more often affected than females, and the right side is involved more often than left. The cause is unknown but thought to be secondary due to a vascular developmental anomaly.
It is rare for all the anomalies of Poland’s syndrome be present in one patient. In our patient, the following anomalies were present:
1. Absence of the right breast.
2. Absence of subcutaneous fat over the right hemithorax.
3. Absence of the pectoralis muscles, as per history given.
4. Absence of serratus anterior and latissimus dorsi muscles.
5. Hypoplasia of the right rib cage accentuating ribs 2 through 5.
6. Right concave scoliosis.
7. Hyperlucency of the right lung.
8. Small right scapula.
Take-home Message
Landmark anatomy is essential in making an accurate diagnosis. X-Rays may identify and characterize specific abnormalities, but x-rays do not display fascial plane anatomy. X-ray imaging displays 70% of an image because 30% is absorbed by the tissues imaged. Magnetic resonance imaging (MRI) may have helped determine the extent to which her muscles were affected. However MRI was not available to our patient. The history she presented with could not be documented as an accurate congenital diagnosis because there were no previous medical records available. Only some of the clinical anomalies of Poland’s syndrome were present in our patient, which is also true in most patients. The absence of the right breast was interpreted as being the cause of the hyperlucent lung. The anomalies that were discovered must be taken into consideration in order to avoid misdiagnosis.
References
1. Radiology 83:63, 1964
2. J. Canad. Assoc. Radio 18:472, 1967
3. Fortschr. Roentgensti 91:488, 1959.
4. Roentgen Diagnosis Vol 1V part 11 Pleura Mediastinum and lungs, Grune and Straton. New York and London 1975 2nd American addition pp16-17
About the Author
James D. Collins, MD, is Professor and General Radiologist in the Department of Radiology at the UCLA David Geffen School Medicine. He formerly served as Director of the required medical student training for the department and President of the James T. Case Radiologic Foundation.
Collins has an extensive background of publications, consultations, and editorial positions, including his current post as the Radiology Editor for the Journal of the National Medical Association. He specializes in bilateral 3-dimensional MRI, MRA, and MRV imaging of the brachial plexus and has been performing those studies since 1985.
















