Publication
Article
Family Practice Recertification
Why Does This Young Woman with Hypertension Have Rib Notching on Her Chest Radiograph?
Author(s):
This 27-year old female medical student with recently diagnosed hypertension is seen following a chest x-ray in work up of a positive PPD. Upon questioning, the patient notes what she described as "gray-out spells" when tired and leg numbness with exercise after periods of sitting.

James D. Collins, MD
History:
This 27-year old female medical student with recently diagnosed hypertension is seen following a chest x-ray in work up of a positive PPD. Upon questioning, the patient notes what she described as “gray-out spells” when tired and leg numbness with exercise after periods of sitting.
Physical Examination:
Notable findings included a blood pressure of 160/110 mm Hg in both upper extremities and diminished pulses in both her legs. Auscultation revealed a systolic heart murmur heard best at the left infraclavicular area and sternal border radiating throughout the precardium and into both carotids and faint intercostal bruits. Examination revealed normal radial and carotid arteries and barely palpable femoral and pedal pulses bilaterally.
Radiological Findings:
The posterior anterior chest radiograph (FIGURE 1) displayed widening of the mediastinum; obscured aortic arch; a “reverse 3 sign” at the level of the left posterior 5th intercostal space on descending aorta, increased lucency marginating the pericardium suggesting mild edema of the adjacent lung, and bilateral rib notching.
The left lateral chest radiograph (FIGURE 2) displayed narrowing of the trachea at the 3rd ribs laterally reflecting dilatation of the brachiocephalic trunk and left common carotid artery; thin subcutaneous tissues, and left ventricular enlargement.
An inverted image (FIGURE 3) of Figure 1 provided a different perspective of the proximal and distal dilated coarctation of the aorta and rib notching of the posterior 6th right rib, heads of the asymmetric clavicles over the posterior asymmetric 3rd ribs. Trachea.
An aortogram, (FIGURE 4), requested by the thoracic surgeon was prior to the surgical correction of the post ductal coarctation, displayed narrowing at the insertion of the ductus arteriosus of aorta and dilatation of the ascending aorta; dilation of the brachiocephalic trunk, internal carotid arteries and subclavian arteries, dilated right thyrocervical trunk, and dilated left intercostal arteries.
A diagram of the diagnostic dilatation in neurofibromatosis compared with those in hyperparathyroidism (FIGURE 5) displayed rib notching caused by abnormal dilated vessels accompanying such entities as coarctation of the aorta (from Isadore Meschan, Synopsis of Analysis of Roentgen Signs in General Radiology, 1976; p 258.
DIAGNOSIS: COARCTATION OF THE AORTA
Discussion:
Coarctation of the aorta is a constriction of the aortic arch, either in its ascending or descending portion . Coarctations can bevategorized into two groups based on the position of the constriction with respect to the ductus arteriosus:
Pre ductal — Usually found in infants and most commonly accompanied by other cardiac defects such as ventricular septal defects, bicuspid aortic valve and patent ductus arteriosus. (1)
Post ducal — Usually seen in adolescents and adults
The clinical presentation of aortic coarctation results from the differential blood flow to various portions of the aorta. Descending on the location of the stricture, there may be, for example, reduced cerebral blood flow as well as poor perfusion of one arm or of both legs.
As a result, dizziness, headache, neck pulsations and/ leg fatigue are common complaints. If problems do not arise in early infancy, symptoms usually do not become obvious until early adolescence. Commonly, systemic hypertension or an abnormal chest radiograph may be the first manifestations of the disorder. On physical examination, diminished pulses in the lower extremities is seen as well as hypertension in the arms and hypotension in the legs.
Complications arising from this anomaly include congestive heart failure as well as either a rupture or dissection of the aorta. Other possible complications include stroke (resulting from a ruptured aneurysm of the circle of Willis) and endocarditis (usually associated with a bicuspid aortic valve).
The radiographic presentation in the adult, post-ductal type, as seen in this case, usually involves findings on routine PA and lateral chest radiographs. The actual coarctation may be displayed. One may also observe the pre-stenotic dilatation of the aortic arch and left subclavian artery and post-stenotic dilatation of the aorta. (2, 3) These compose the often described reverse “3” configuration along the left mediastinal border in the coarctation.
Other findings result from increased collateral flow. This includes dilatation of the internal thoracic artery, brachiocephalic and thyrocervical trunk arteries. Rib notching, observed in this case, is a common finding in this condition. It results from the pressure of dilated intercostal arteries on the inferior margins of the ribs. This is more obvious in the AP view and usually involves the fourth to eighth ribs. The notching is usually symmetric. If it is isolated to the right side, the stenosis may be proximal to the origin of the left subclavian artery. Therefore collateral flow must develop from the adequately supplied right subclavian artery through the right rib collaterals to the descending aorta.
If notching is isolated to the left side there must be higher pressures in the left subclavian artery than the right, to have increased flow from the left through left rib collaterals to the descending aorta. This could occur if there is an aberrant left subclavian artery proximal to the right with the coarctation proximal to the right subclavian artery, and distal to the left subclavian artery.
Uniform rib notching can occur in other disorders, which produce increased flow to the descending aorta over the subclavian arteries or increased flow through the rib collateral secondary to lung disease. These disorders include:
• Blalock-Taussig, anastomosis
• Subclavian occlusion
• Pulmonary atresia
• Post thoracotomy
Superior rib notching or thinning, also affecting ribs four to eight, is most commonly the result of chronic paralytic poliomyelitis or neurofibromatosis.
One can diagnose coarctation on plain radiographs but angiography, as performed in this case, can aid in differentiation of a dilated aorta from mediastinal masses as well as aid the surgeon in pre-operative assessment. (2)
FIGURE LEGENDS


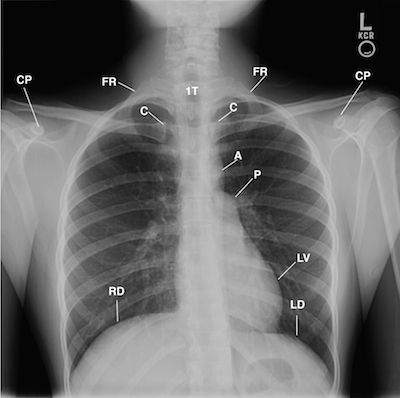
FIGURE 1 is the posterior-anterior chest radiograph displays the forward elevated right shoulder as compared to the left shoulder; widen mediastinum secondary to dilated great vessels (not labeled); asymmetric anterior rotated heads of the clavicles (C) over the posterior 3rd ribs (not labeled); increased density of the pulmonary vessels along the right heart border accentuating increased radiolucency between the right lung and pericardium (not labeled) reflecting the pulsating heart against an edematous right lung, and left ventricular enlargement (LV). Coarctation (CO), FIRST RIBS (FR), LEFT (LEFT AND RIGHT HEMIDIAPHRAGM ( LD, RD), LEFT VENTRICULAR ENLARGEMENT (LV), TRACHEA (T), SMALL ARROWS ( NOTCHING OF THE RIBS).


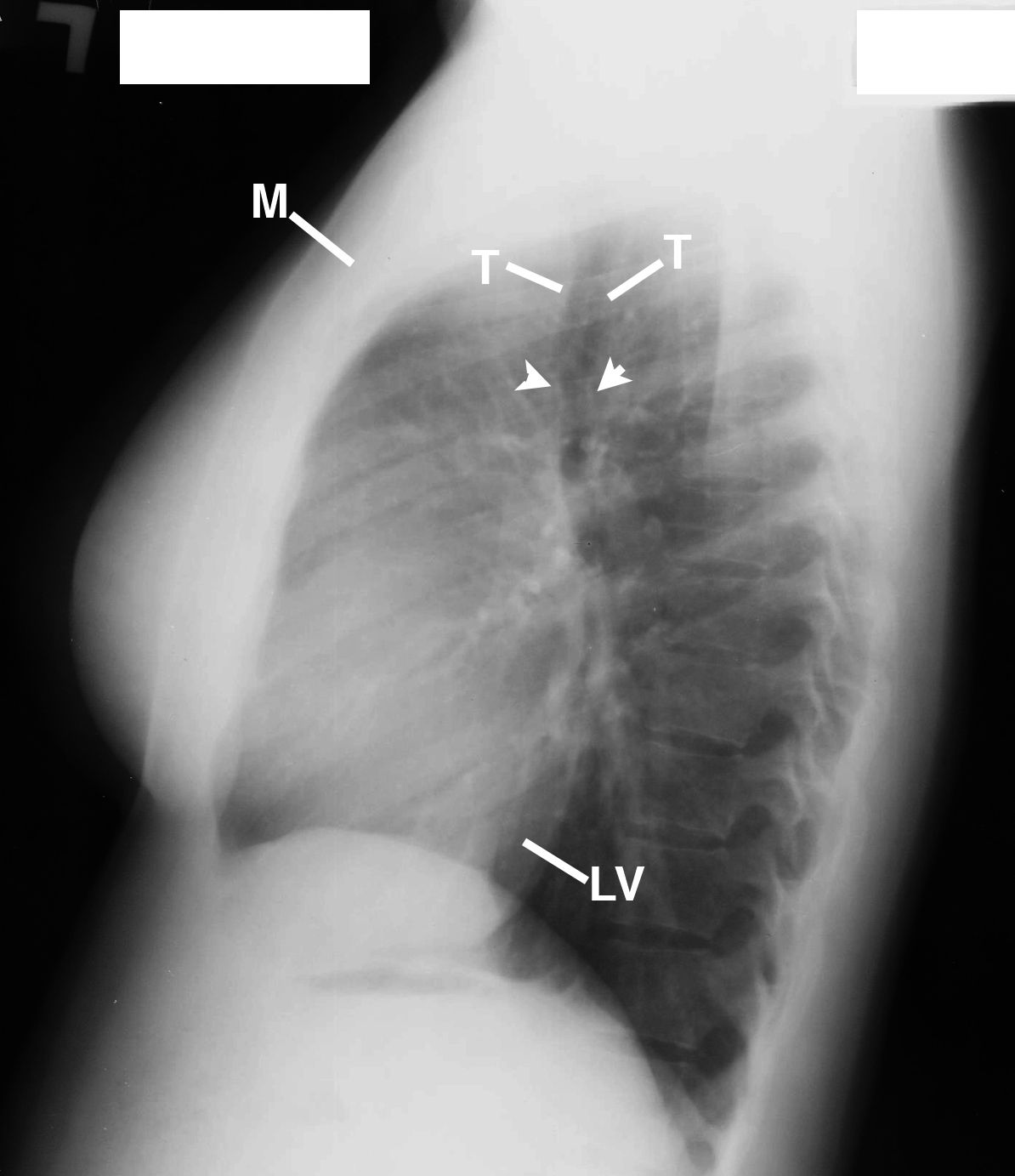
FIGURE 2 is the left lateral chest radiograph that displays narrowing of the trachea secondary to the coarctation (2 arrows), Left ventricular enlargement (LV), Manubrium (M), TRACHEA (T).


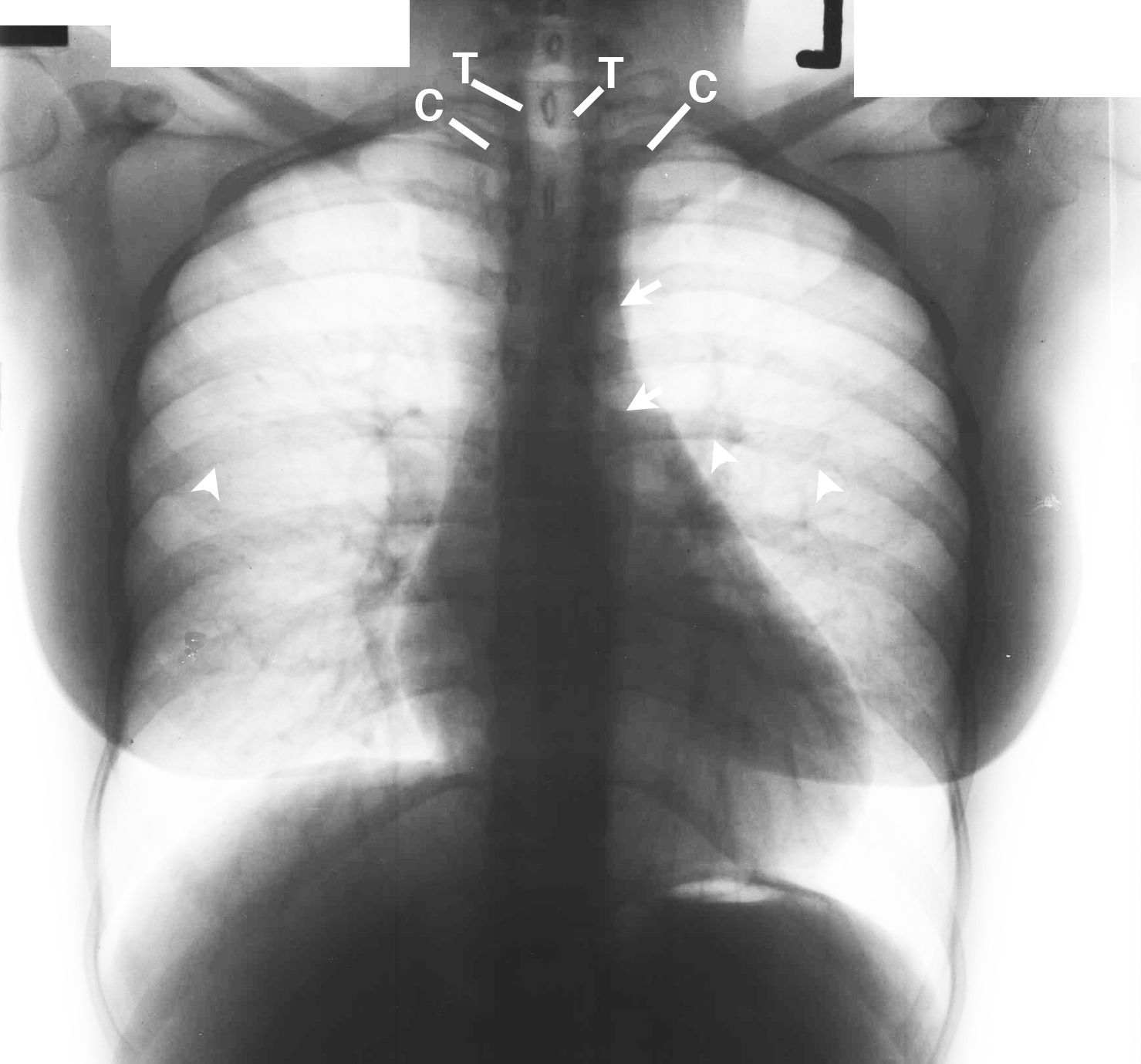
FIGURE 3 is the inverted image of Figure that gives a different perspective of the proximal and distal dilated coarctation of the aorta (2 arrows) and rib notching of the posterior 6th right rib (single arrow). Heads of the clavicles (C) over the posterior asymmetric 3rd ribs (not labeled), Trachea (T).


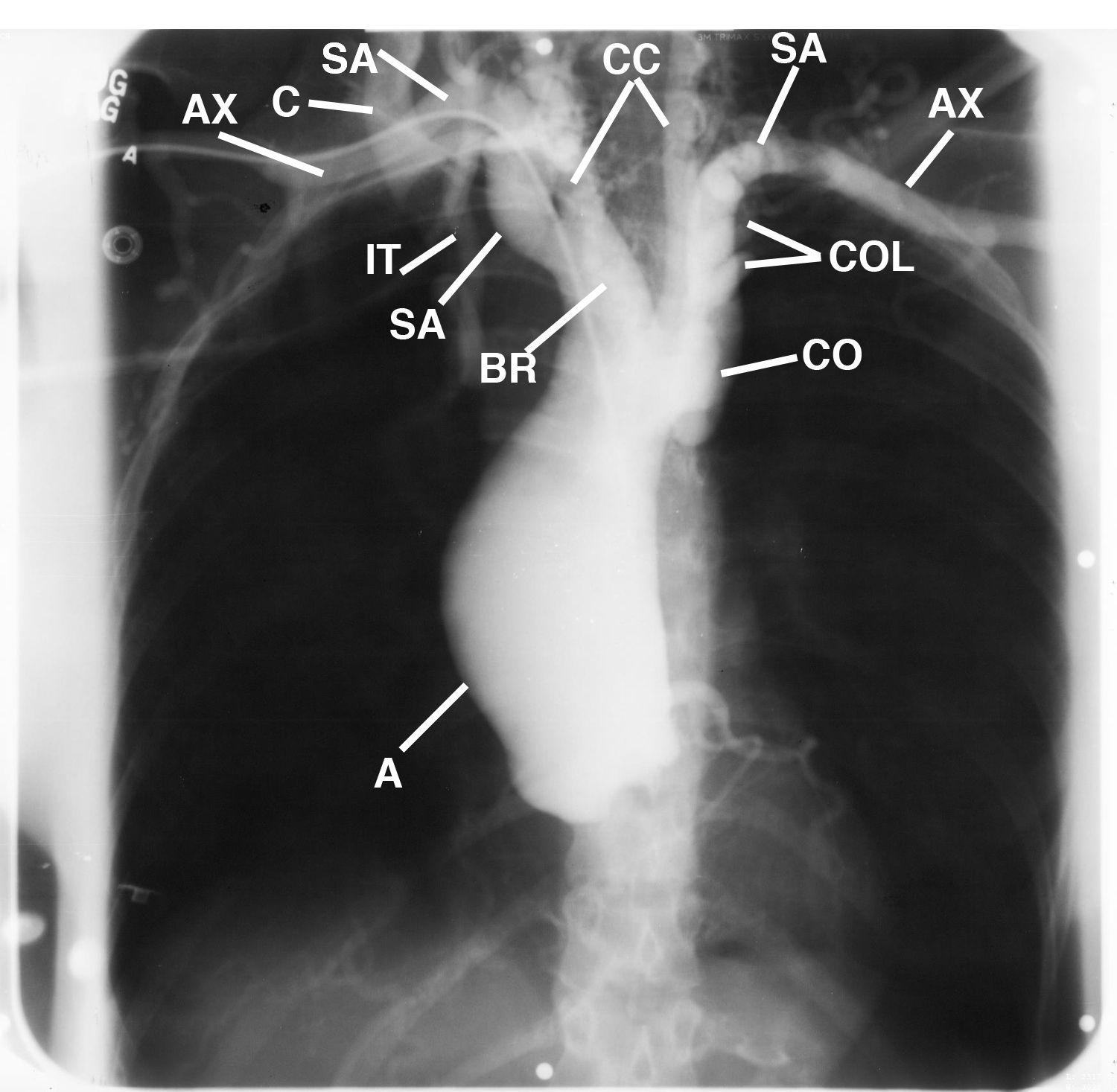
(FIGURE 4) This percutaneous aortagram from a right axillary artery approach displays the aneurismal dilatation of the ascending aorta (A), axillary artery (AX), right clavicle (C), coarctation of the proximal descending aorta with the dilated ascending aorta (CO), dilated brachiocephalic trunk (BR), origin of the dilated right common carotid artery ascending from the brachiocephalic trunk and the left common carotid from the arch of the aorta (CC), dilated first division of the right subclavian artery (SA), right internal thoracic artery (IT), thyrocervical trunk (not labeled), dilated first division of the left subclavian artery (SA) overlaying dilated left posterior intercostal arteries (COL). .


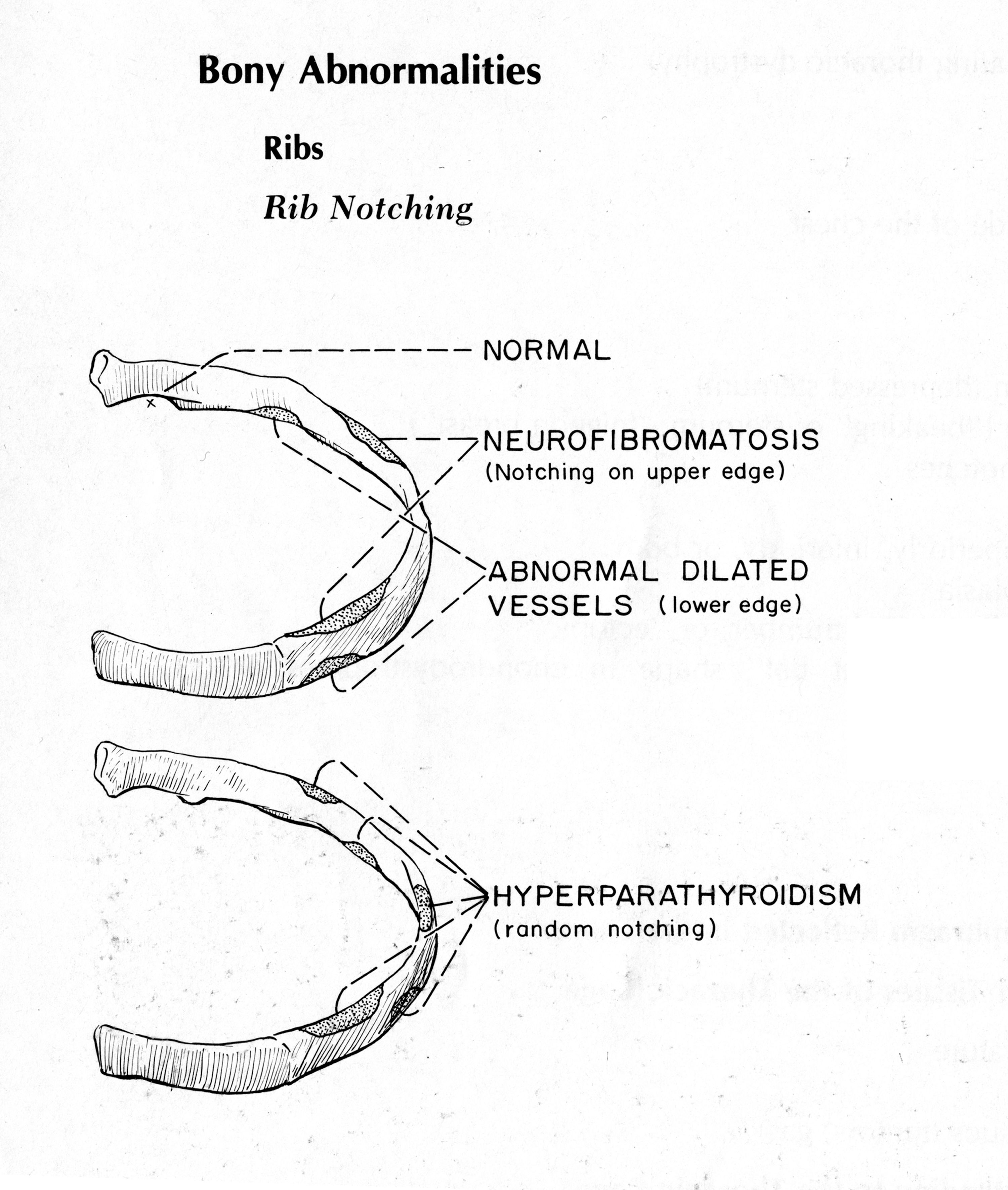
Figure 5 is a diagram of the diagnostic dilatation in neurofibromatosis compared with those in hyperparathyroidism. Also displayed are the rib notching caused by abnormal dilated vessels accompanying such entities as coarctation of the aorta (from Isadore Meschan, Synopsis of Analysis of Roentgen Signs in General Radiology, 1976; p 258.
TAKE HOME MESSAGE
Common radiologic signs of coarctation of the aorta are often diagnosed on plain chest radiographs. Since 30% of the x-ray beam is absorbed by the tissues through which the beam passes, only 70% of the image is displayed on the plain chest radiograph, which makes it difficult to display the findings on our manuscript. Magnetic resonance imaging (MRI) would have displayed fascial planes and the coarctation without confusion.
REFERENCES
1. Caffey, John; Pediatric X-ray Diagnosis, 1961 pgs. 470-72.
2. Perloff, Joseph; The Clinical Recognition of Congenital Heart Disease, 4th edition 1978, pgs 132-35.
3. Shanks, Cochrane and Peter Kerley; A Textbook of X-ray Diagnosis.
4. Meschan, Isadore: Synopsis of Analysis of Roentgen Signs in General Radiology. 1976 by W. B. Saunders Company.
About the Author
James D. Collins, MD, is Professor and General Radiologist in the Department of Radiology at the UCLA David Geffen School Medicine. He formerly served as Director of the required medical student training for the department and President of the James T. Case Radiologic Foundation.
Collins has an extensive background of publications, consultations, and editorial positions, including his current post as the Radiology Editor for the Journal of the National Medical Association. He specializes in bilateral 3-dimensional MRI, MRA, and MRV imaging of the brachial plexus and has been performing those studies since 1985.